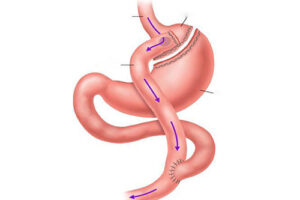
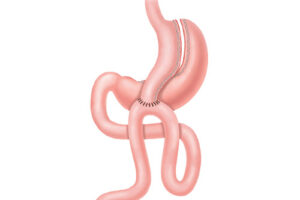
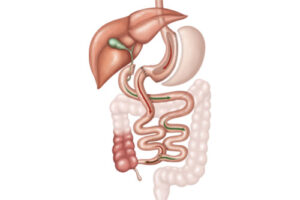
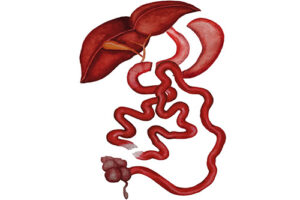
In this application, a tube stomach surgery is applied first. Here, the stomach volume is left a little wider than the tube stomach. Then the junction of the small intestine and large intestine is found (ileocecal junction). Starting from this junction, the small intestine is counted as centimeter backward. It is reached from the ileocecal junction 100 - 120 cm. This point is marked. (Depending on the patient, this part can be 80-200 cm). Continuing to count, reach 250-270 cm from the ileocecal junction. In other words, it will be 150 cm higher than the place where we made the sign. (Depending on the patient, this distance can be 50-150 cm) When it reaches the 100-120 cm up to the marked place and 150 cm from there, that is a total of 250-270 cm, this small intestine is partially cut and divided into two. Now we have 2 small intestine ends. The lower end, which is calculated from the ileocecal junction, is drawn towards the lower part of the stomach. The end of the 250-270 cm intestine up to the ileocecal junction is aimed to be mouthed with the lower part of the stomach. For this purpose, the stomach and small intestine are mouthed with a window opened in a suitable area in the lower part of the stomach and some of the food is passed through this 250-270 cm part. However, the upper end of the small intestine that we cut and cut from 250-270 cm remains in our hands. Here comes stomach acid, bile, pancreatic fluid, etc. At this end, we initially calculate from the ileocecal junction and mark 100-120 of the small intestine. It is mouthed with cm part.